The 2026 Guide to Negotiating Medical Bills: How to Save 40% Using “CPT Codes” (Step-by-Step)

The Chargemaster Illusion: Why Published Prices Are Negotiating Anchors
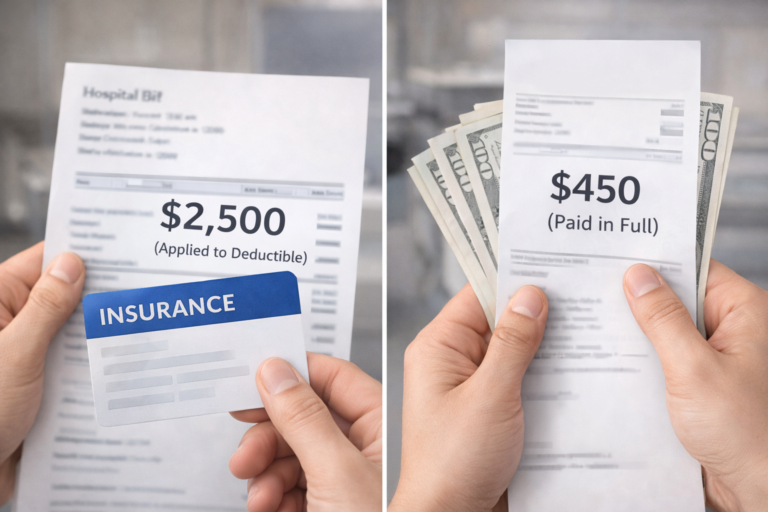
Consider the behavioral economics at play. A hospital posts a $2,500 charge for a routine consultation. Most patients treat this figure as immutable—a regulatory mandate rather than what it actually is: an opening position in a negotiation.
This is not a moral failing on anyone’s part. It’s an information asymmetry, and information asymmetries create arbitrage opportunities. The question is whether you’re on the profitable side of that equation.
Several years ago, I received a laboratory charge 5× the regional benchmark. Rather than accepting the premise, I reverse-engineered the pricing mechanism. What I discovered was a reimbursement architecture that rewards opacity and penalizes the uninformed.
What follows is a systematic approach to price discovery and leverage creation, calibrated to 2026 regulatory frameworks.
Strategic Move 1: Obtain Granular Transaction Data
The summary statement you receive is strategically vague—designed for payment, not analysis. Line items like “Pharmacy Services: $800” offer no forensic utility.
As of February 2026, coinciding with REAL ID enforcement, hospitals have tightened identity verification and billing processes significantly. This means your request for documentation now carries additional regulatory weight—use it.
Your first tactical objective is to request the underlying data structure. Use this specific language:
“I require a complete Itemized Statement with CPT codes for all rendered services. Payment processing will commence upon verification of billing codes against procedure documentation.”
The strategic value: Current Procedural Terminology (CPT) codes are the universal language of medical billing. Each 5-digit code maps to a specific, standardized service. Without this granularity, you’re negotiating in the dark.
Strategic Move 2: Conduct a Forensic Audit (The Error Arbitrage)
Once you have code-level visibility, your next move is error detection. The assumption that hospital billing systems operate with high fidelity is empirically false.
I monitor billing pattern analysis through communities like r/HospitalBills to identify systemic vulnerabilities. A recent case study is instructive:
A patient presented with a lower extremity injury. The itemized statement included CPT 81025—a urine pregnancy test. The patient was male.
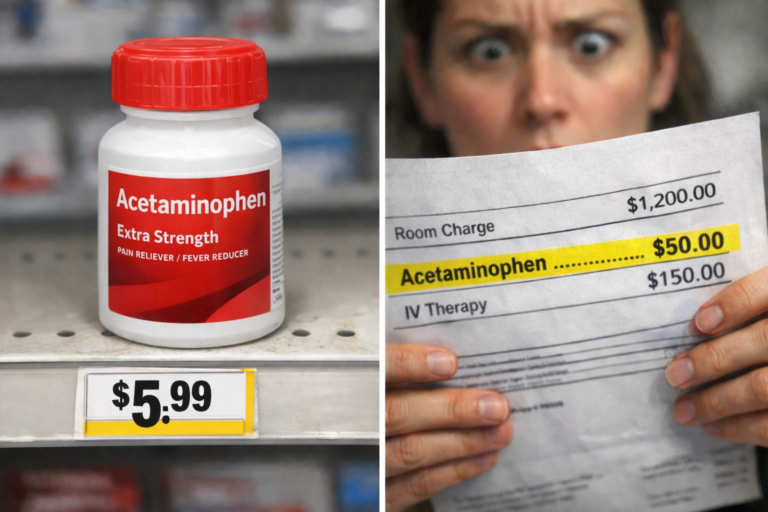
This isn’t anecdotal. Duplicate charges, miscoded procedures, and “upcoding” (billing a higher-complexity service than delivered) appear in approximately 80% of hospital bills according to billing auditor analysis. Each unchallenged error represents a direct wealth transfer from you to the billing entity.
Strategic Move 3: Establish the True Market Clearing Price
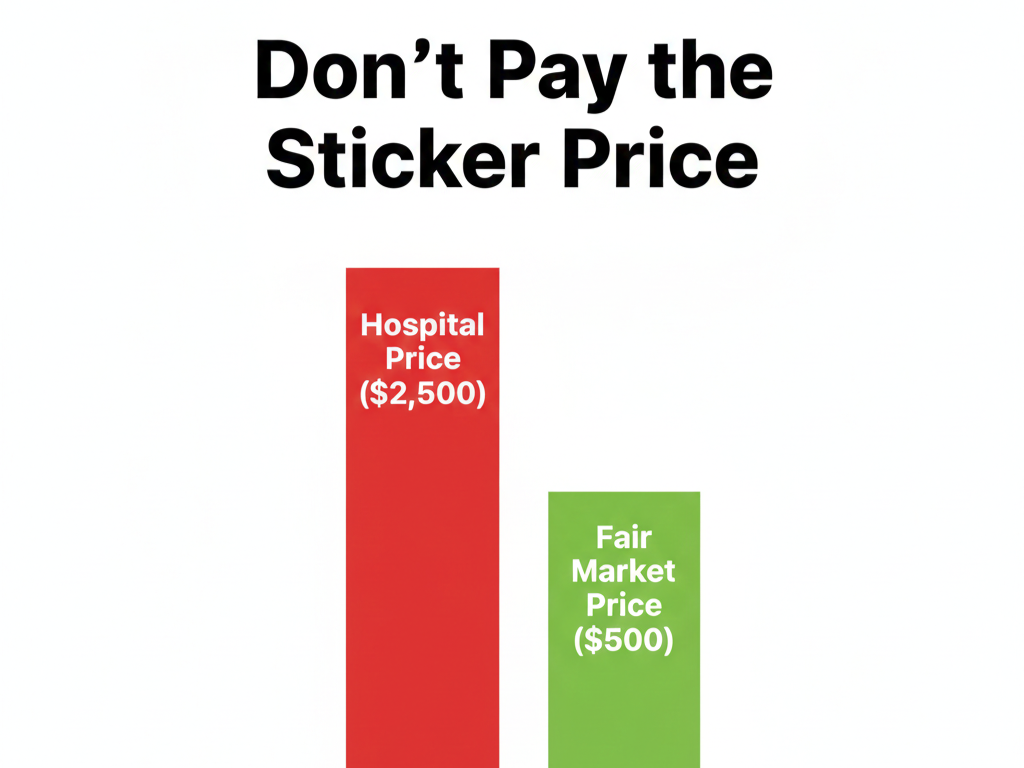
Hospitals maintain a “Chargemaster”—essentially a list price that functions as a negotiating ceiling. Insurance carriers never pay these rates. They’ve already negotiated discounts ranging from 40-80% below list.
If you’re self-pay, you should command similar economics. Here’s the price discovery protocol:
- Access benchmarking platforms: Healthcare Bluebook or FAIR Health Consumer
- Input the specific CPT code and your geographic market (ZIP code)
- Extract the regional median transaction price
If your bill shows $500 for a procedure with a $100 regional median, you now possess leverage. The optimal move: offer immediate cash settlement at 120-150% of fair market value. The billing department faces a decision tree: accept $150 today with zero collection friction, or pursue $500 through collections channels where they’ll eventually sell the debt for $50-100.
The rational actor accepts your offer.
If direct negotiation feels daunting, consider leveraging AI-powered medical bill auditing tools. These platforms automate error detection and generate counter-offer scripts based on regional pricing data. (I’ll be covering the top 3 cost-effective Medical Bill Auditors for 2026 in my next post.)
Advanced Tactic: The Structural Subsidy Layer
Before executing even a negotiated settlement, examine the subsidy architecture. Non-profit hospitals (approximately 58% of U.S. acute care facilities) are legally required to maintain Financial Assistance Policies (FAP) under IRC Section 501(r).
2026 income thresholds have been adjusted for inflation. Even employed individuals with seemingly “disqualifying” incomes may be eligible for partial discounts (20-60% reduction) if the medical expense exceeds certain income-to-debt ratios.
The key document: search the hospital’s website footer for their “501(r) Financial Assistance Application” or “Charity Care Policy.” This is frequently de-emphasized in their information architecture—but it’s legally mandated to exist.
This is how we survive the system. — Alex
⚠️ Operational Disclaimer
This analysis is provided for strategic educational purposes and does not constitute financial, legal, or medical counsel. I function as a healthcare navigator synthesizing 2026 regulatory frameworks—not as a licensed attorney or certified financial planner.
Billing policies exhibit significant variance by jurisdiction and institution. Verify all tactics against your specific provider agreements and state regulations. In medical emergencies, clinical care takes absolute precedence over billing optimization.