The PBM Arbitrage: Decoupling Your Prescription Costs from Insurance Logic

The Decoupling of Cost and Value
In a rational market, insurance functions as a hedge against catastrophic financial risk. In the U.S. pharmaceutical sector, however, insurance frequently operates as a value extraction mechanism.
Consider the mechanism known as the “Copay Clawback.” Your insurer charges you a $30 copay for a generic medication that costs the pharmacy $2 to dispense. The $28 differential doesn’t accrue to the pharmacy—it’s “clawed back” by the PBM (Pharmacy Benefit Manager).
You’re not purchasing the drug. You’re paying a premium for the “privilege” of presenting your insurance card. This represents a market inefficiency that informed consumers can exploit through regulatory arbitrage.
What follows is the protocol to dismantle this pricing architecture and access the true market clearing price.
The Intermediary Layer: Decoding PBM Pricing Algorithms
Your medication price is determined by opaque algorithms controlled by Pharmacy Benefit Managers (PBMs)—intermediaries like CVS Caremark, Express Scripts, and OptumRx. They negotiate rebates with manufacturers but rarely transmit those savings to end consumers.
As of February 2026, following updated CMS transparency mandates and REAL ID verification integration at pharmacy points of sale, PBMs are now required to disclose certain pricing tier structures—though the disclosure mechanisms remain deliberately complex.
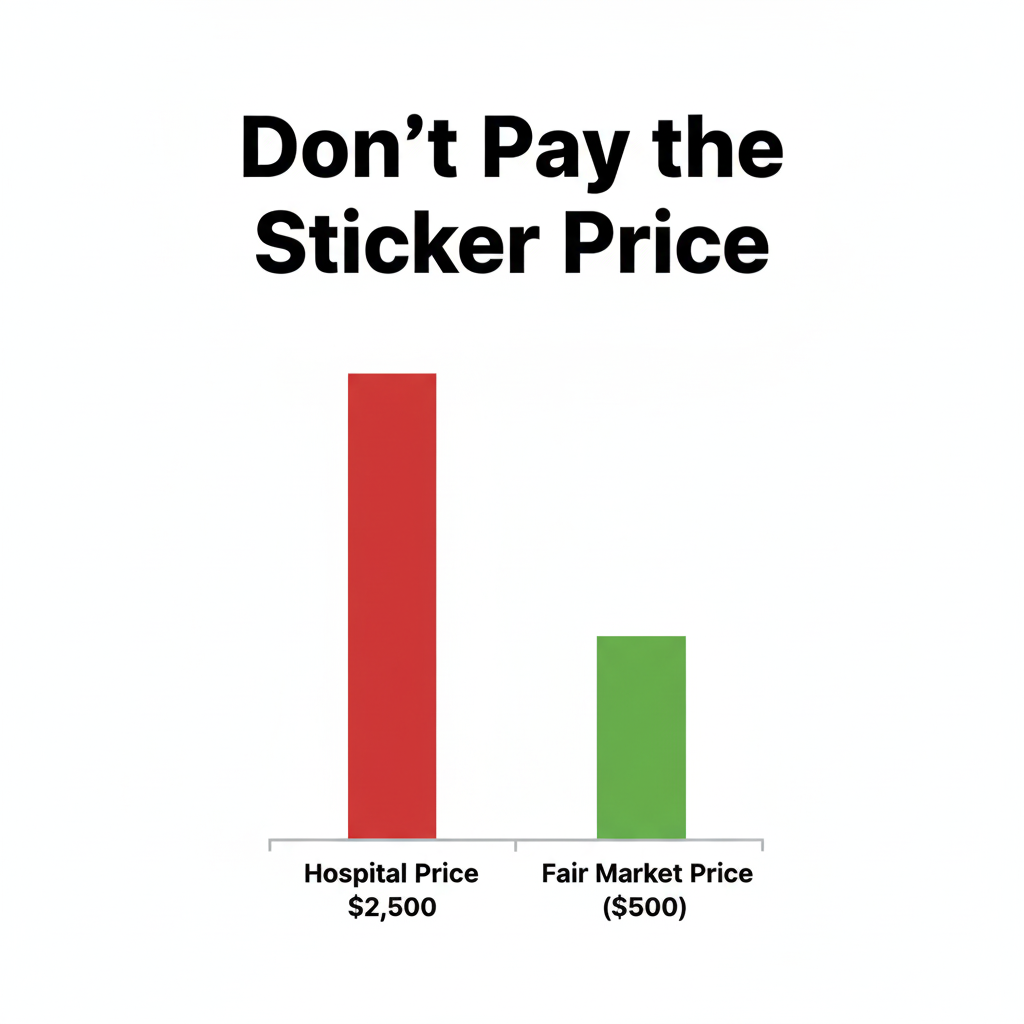
This creates systematic pricing distortion. A single drug may have three simultaneous price points at the same counter:
- The Chargemaster Price: Inflated “list price” for uninsured patients ($200)
- The Insurance Negotiated Rate: What your insurer actually reimburses ($100)
- The True Market Price: Actual acquisition cost plus minimal margin ($15)
Your strategic objective is to access the third tier.
Strategic Move 1: The Cash Bypass Protocol
Do not reflexively present your insurance card. In approximately 40% of generic prescription fills, the cash price (leveraging discount network infrastructure) is lower than your insurance copay.
Historically, pharmacists operated under “Gag Clauses” that contractually prohibited them from volunteering this price differential. While legislation has nominally banned these clauses, institutional inertia persists. You must initiate the inquiry.
The Verbal Protocol: “I’m requesting a price comparison query. Please process this prescription at cash price using [GoodRx / SingleCare] discount code. If the net cash price is lower than my $20 copay, I’ll pay out-of-pocket for this transaction.”
Deductible Consideration: Cash payments typically do not count toward your annual insurance deductible. This is a calculated tradeoff. If your deductible is $5,000 and you maintain low utilization, optimizing immediate cash flow is often statistically superior to accumulating deductible credits you’re unlikely to trigger.
Strategic Move 2: The Direct Supply Chain Architecture
The most significant market disruption in 2026 is the maturation of the Cost-Plus Distribution Model.
Platforms like Mark Cuban Cost Plus Drug Company have eliminated the PBM intermediary layer entirely. Their pricing algorithm is transparent by design: Manufacturing Cost + 15% Markup + $3-$5 Pharmacy Processing Fee.
I conducted pricing analysis on Imatinib (a leukemia medication). Traditional retail pricing exceeds $2,000 per fill. Cost Plus pricing: under $20. This isn’t a promotional discount—it’s the elimination of an artificial market friction.
The Execution Protocol: Before filling any chronic medication, cross-reference the generic molecule name on direct-to-consumer platforms. If the price differential exceeds 50%, transfer the prescription immediately.
If navigating prescription transfers and price comparisons feels overwhelming, consider using prescription price optimization tools that automate this analysis. (I’ll be evaluating the top 3 Prescription Cost Transparency Platforms for 2026 in my next breakdown.)
Strategic Move 3: Therapeutic Interchange (The Molecular Substitution)
Physicians often prescribe the most recent molecule in a therapeutic class due to pharmaceutical detailing (industry marketing). However, an earlier-generation drug in the same pharmacological class may achieve 95% therapeutic equivalence at 10% of the cost.
This is termed Therapeutic Interchange.
If a prescribed brand-name medication is cost-prohibitive, avoid asking: “Is there a generic available?” (One may not exist yet). Instead, query: “Is there a therapeutic equivalent in an earlier drug class that is available generically?” You’re requesting a different molecular structure that achieves the same clinical endpoint.
Volatility is a risk. Opacity is a trap. — Alex
⚠️ Operational Disclaimer
I function as a strategic navigator analyzing pharmaceutical market mechanisms—not as a licensed pharmacist or physician. The strategies outlined (Cash Bypass Protocol, Cost-Plus Architecture, Therapeutic Interchange) are financial optimization tactics based on 2026 market structures.
Clinical Imperative: Never modify dosage, discontinue medication, or substitute therapeutic agents based on cost considerations without consulting your prescribing physician. “Therapeutic Interchange” requires a new prescription from a licensed provider. Medication pricing exhibits daily volatility based on supply chain dynamics. Always verify final transaction costs at point of sale.